
Most health systems don't have an AI readiness problem. They have a sequencing problem. The budgets exist, the board has signed off, and the vendor conversations have been running for months. What stalls deployment is the absence of a credible operational path from approval to production: one that delivers measurable results without requiring a three-year transformation program before anything works.
AI in healthcare is not a single technology or a single decision. It spans revenue cycle management, scheduling optimization, diagnostic imaging, and advanced clinical applications with wildly different regulatory complexity, data requirements, and deployment timelines. The health systems that move fastest resist the pressure to deploy everything simultaneously. They start where the operational infrastructure is already strongest, prove the model, and expand from there. That's the approach that defines AI in healthcare operations at the health systems achieving production results today.
This guide gives you that path: a 90-day framework built around the use cases with the shortest time to production value, structured so that the operational foundation you build in the first 30 days supports everything you deploy in days 31 through 90 and beyond.
The most durable AI deployments in healthcare begin with administrative operations, not clinical workflows. That's not a concession; it's a structural advantage. The administrative burden in healthcare is where the volume is highest, the documentation is richest, and the feedback loops are tightest — exactly the conditions that make AI deployable fast. Administrative workflows also generate the data infrastructure that more complex clinical applications depend on.
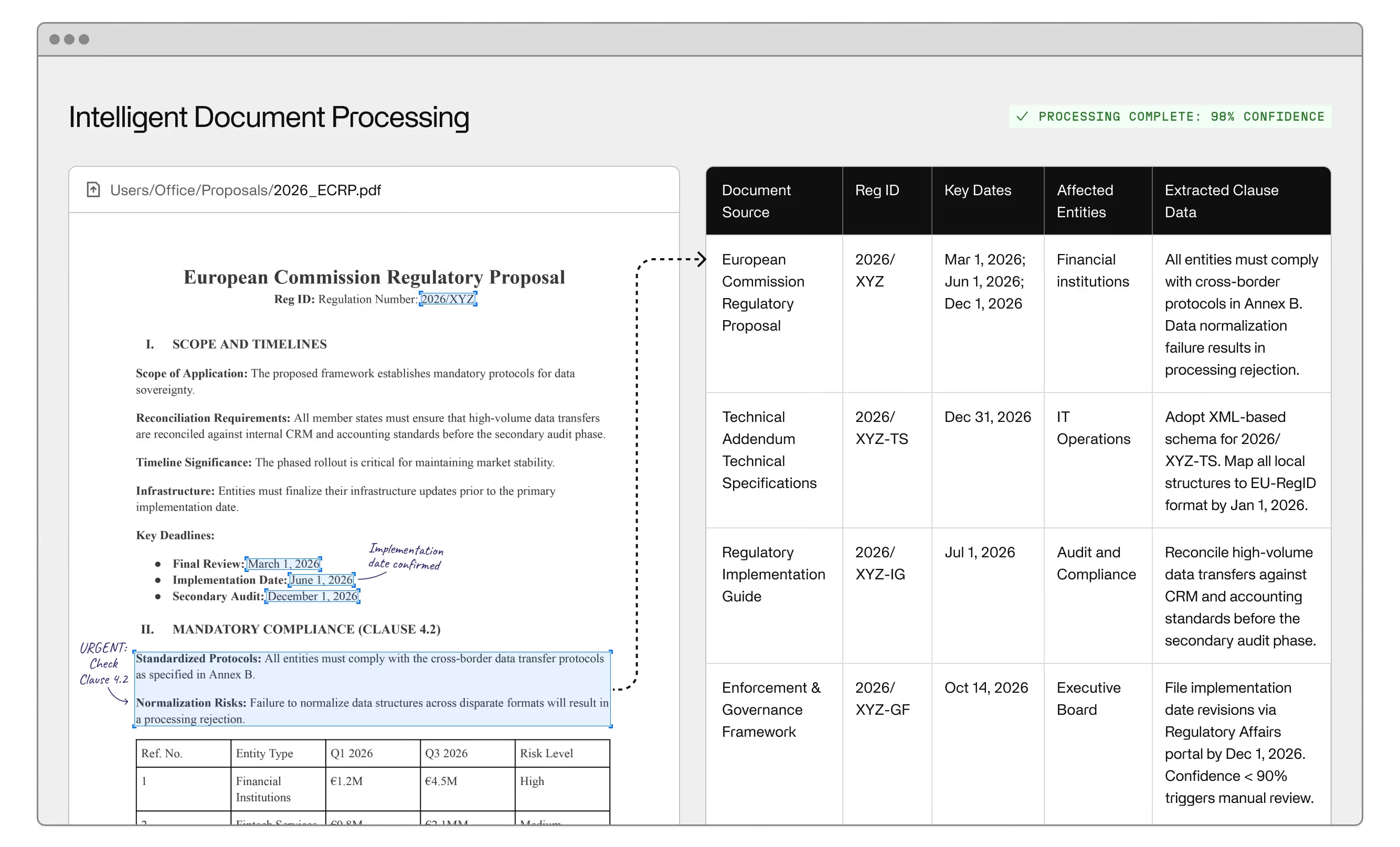
Medical coding is the clearest example. Health systems process thousands of encounters daily, each requiring accurate assignment of codes against patient data, medical history, and clinical documentation. Manual coding is slow, error-prone, and directly connected to revenue cycle performance. AI-assisted coding, already in production at health systems that report 30–50% reductions in coding turnaround time, is an ideal first deployment because the quality criteria are objective, the feedback loop is tight, and the ROI is measurable in weeks, not quarters.
Revenue cycle management follows the same logic. Claims processing, denial management, prior authorization, and billing accuracy are all tractable problems for AI trained on structured clinical and financial data. The integration points are well-defined, and you're not asking a model to make a clinical judgment. You're asking it to extract, classify, and route information it can be trained to handle reliably.
Patient engagement is the third early-deployment priority. Scheduling optimization, appointment reminders, and personalized care communications all operate on structured clinical data and produce outcomes you can measure within weeks. Automated appointment scheduling and basic triage handling are now standard infrastructure at health systems that have moved past the pilot stage: they reduce inbound call volume to the contact center, improve patient engagement scores, and free clinical staff for higher-complexity interactions.
None of this is the frontier of what AI in healthcare can do. Drug discovery, precision medicine, and robot-assisted surgery represent genuinely transformative clinical applications that require the operational maturity the first 30 days are designed to build.
The deployment failures that define AI in the healthcare industry share a common structure: they start too big, skip the data readiness work, and underestimate what clinical staff actually need to adopt new systems.
Data readiness is the most common breaking point. Electronic health records are the canonical source of patient data, but EHR data is rarely clean, consistently structured, or accessible in the format AI models need. Medical history records span decades, multiple systems, and inconsistent documentation standards. Before any model touches clinical data, you need a data governance framework that defines what data is accessible, how it's labeled, who can access it, and how it's versioned. Health systems that skip this step deploy models that perform well on training data and fail in production.
FDA regulatory requirements add complexity to any deployment touching diagnostic or clinical decision-support functionality. The FDA's framework for AI/machine learning-based software as a medical device (SaMD) applies to tools that inform clinical decisions, and the regulatory pathway for these tools is materially longer and more demanding than for administrative AI applications. ChatGPT and general-purpose large language models are not FDA-cleared for clinical use. Deploying them in clinical workflows without proper validation creates both patient safety and liability exposure. The FDA has cleared specific AI tools for defined diagnostic tasks, but those clearances apply to specific models, not AI in general.
The risks of AI in healthcare also include algorithmic bias. AI systems trained on historically unrepresentative patient data can perform systematically worse for certain demographic groups, an issue the FDA now requires developers to address in high-risk clinical AI submissions. This is not an abstract concern: studies have documented differential performance in AI-assisted diagnosis across race, sex, and age. Operational deployments need explicit bias monitoring built in from the start, not added as an afterthought.
Health worker adoption is the third failure mode. The best AI-powered tools fail if the people expected to use them don't trust the output or can't integrate it into existing workflows. Clinical staff who experienced the disruption of EHR implementation in the 2010s approach new systems with earned skepticism. Change management, workflow integration, and clear communication about what the AI does and doesn't do are not soft requirements. They determine whether a technically sound deployment actually produces operational results.
The first 30 days are not about deploying AI. They're about building the infrastructure that makes AI deployable and getting one high-confidence, high-volume use case into production to demonstrate that the program is real.
Start with a data and systems audit. Map what data exists, where it lives, and what state it's in. EHR systems, billing platforms, scheduling tools, and contact center data are the core sources. The audit should answer three questions: what data is accessible today, what requires remediation before it can be used, and what integration work is needed to connect your tooling to source systems. HIPAA-certified environment requirements apply from day one. Every data flow needs to be mapped against your compliance architecture before it goes into a model pipeline.
Alongside the audit, select the first production use case. Medical coding automation is the strongest choice for most health systems: the data is structured, the quality criteria are objective, and the business case is unambiguous. If revenue cycle is a higher operational priority, automated claims processing or prior authorization is a credible alternative. The decision criteria are the same. Choose the use case where you have the cleanest data, the clearest success metrics, and the most motivated operational owner.
By Day 30, the target is a single AI application in production, a data governance framework documented and signed off, and a deployment team that has run the first integration cycle with your EHR. That's a foundation. Everything from Day 31 forward builds on it.
With the administrative foundation in place, the second phase introduces patient-facing AI applications and begins the groundwork for clinical decision support.
Patient engagement is the natural expansion. An AI-powered chatbot handling appointment scheduling, prescription refill requests, and basic triage queries reduces contact center volume while improving response times for patients. The data infrastructure from phase one (clean EHR integration, HIPAA-compliant access controls, connection to scheduling systems) is exactly what patient-facing AI applications need. Deploy this layer now and instrument it to capture engagement data that will inform outreach communications in phase three.
Predictive analytics for capacity planning and resource allocation is the second expansion priority. Machine learning models trained on historical admissions data, staffing patterns, and seasonal demand signals can forecast patient volume, flag capacity constraints, and support labor scheduling decisions. These are not clinical AI applications. They don't touch diagnosis or treatment, but they directly affect clinical outcomes by ensuring the right staffing levels are in place before demand peaks rather than in response to them. Health systems that deployed predictive analytics tools during the COVID-19 pandemic to manage surge capacity demonstrated what this capability looks like in production under pressure.
Virtual health assistants for post-discharge follow-up and chronic disease management also belong in this phase. These applications use clinical records from the EHR to deliver personalized care communications: medication reminders, symptom check-ins, care plan adherence support, without requiring clinical staff time for routine outreach. Patients with kidney disease or diabetes management needs see measurably better adherence outcomes when follow-up is consistent. AI makes consistency operationally feasible at scale.
By Day 60, you should have three to four applications in production, a functioning data pipeline from your EHR to your AI tooling, and the first performance data from your phase one deployment. That data is your evidence base for the clinical AI applications coming in phase three.
The third phase introduces the AI applications with the longest clinical validation requirements and the highest operational upside: diagnostic imaging, clinical decision support, and the foundations of precision medicine.
Medical imaging is where FDA-cleared AI tools have the strongest commercial footprint. Diabetic retinopathy screening (where AI analysis of retinal images can detect early-stage disease with accuracy comparable to specialist review) is approved, deployed, and producing outcomes at health systems globally. FDA-cleared tools for CT scan and X-ray interpretation, covering pulmonary nodule detection, intracranial hemorrhage identification, and pneumothorax flagging, also exist for specific applications. These tools are not general-purpose diagnostic AI. They are narrowly scoped, validated for specific tasks, and designed to flag findings for clinician review rather than replace it.
The deployment model for diagnostic AI is different from administrative AI. You're not just integrating data and setting performance thresholds. You're embedding a clinical decision-support system into workflows that carry direct patient safety implications. That means clinical validation against your own patient population, workflow integration with your radiologists or specialist teams, and explicit protocols for how AI-generated findings are reviewed and acted on. ChatGPT and general-purpose LLMs have no place in this workflow. The tools that belong here are purpose-built, FDA-cleared, and validated on representative populations, including validation for performance across demographic groups to address the algorithmic bias risks documented in medical imaging AI.
Robot-assisted surgery and precision medicine applications (AI-driven treatment selection connecting molecular data to individual patient profiles) are on the horizon of what health systems need to plan for rather than deploy in a 90-day cycle. The genomics infrastructure that supports these applications takes longer to build than 90 days. What the third phase does is establish the clinical AI governance structure and the model validation framework these applications will require when they're ready.
Personalized medicine as an operational concept, tailoring treatment decisions to individual patient profiles using AI-synthesized data, is not science fiction, but it is not a Day 90 deliverable. The traditional medicine paradigm, which relies on population-level evidence applied uniformly, is being supplemented by AI tools that can identify which patients are likely to respond to which interventions. That shift happens at the infrastructure level before it becomes visible at the point of care. It requires the data architecture and model governance that the traditional medicine-to-AI transition depends on. The 90-day program you're building now is that foundation.
The 90-day program produces a running AI operation, not a finished product. What happens after Day 90 determines whether the investment compounds or plateaus. The goal is not to streamline operations through a single deployment; it's to build the infrastructure that makes every subsequent deployment faster, more accurate, and more deeply embedded in clinical practice.
The first post-90-day discipline is model monitoring. AI systems in production degrade when the data distribution they're deployed against shifts away from the data they were trained on. Patient population changes, EHR updates, coding standard revisions: all of these can cause a model that performed at 95% accuracy at launch to drift toward 85% over 18 months without any visible signal to the people using it. Monitoring needs to be instrumented from deployment, not retrofitted when performance problems become visible.
The second discipline is feedback loop management. Every AI application in your stack should have a defined mechanism for capturing clinician and operational staff feedback on AI outputs: cases where the model was wrong, cases where the output was technically correct but clinically unhelpful, and cases where the model's recommendation conflicted with practitioner judgment. This feedback is training data for the next model iteration. Health systems that build feedback infrastructure from the start produce better models over time; those that don't produce static tools that become gradually less useful.
The third discipline is honest integration with traditional medicine workflows. AI in healthcare does not replace clinical judgment. It changes what clinical judgment is applied to. The most productive framing for clinical staff is not that AI does the job faster, but that AI handles the high-volume, high-frequency tasks that shouldn't require specialist attention, freeing practitioners for the complex, ambiguous, high-stakes cases where human judgment is irreplaceable. That framing needs to be built into how you communicate the program internally from day one, not introduced as a defensive move after adoption problems emerge.
Health systems that deploy AI in healthcare as a cost reduction exercise tend to underinvest in the human infrastructure (training, change management, feedback mechanisms) that determines whether the technology actually produces clinical and operational value. The ones that treat the operational investment as a capability build, with AI as the accelerant rather than the destination, are the ones that are still expanding their programs three years after the first deployment. The same phased logic applies across operational domains — the AI demand forecasting implementation framework follows an identical build sequence for supply chain and capacity planning teams running a parallel deployment.
Ready to move from planning to production? Invisible deploys HIPAA-certified AI for health system operations — from revenue cycle and scheduling to clinical decision support. Get started.
The first administrative AI application (revenue cycle automation or claims processing) can reach production within 30 days for health systems with clean EHR data and defined integration points. Clinical AI applications with regulatory review requirements take significantly longer, typically six to eighteen months depending on clinical validation scope. The 90-day framework gets three to four administrative and patient-facing tools into production while laying the groundwork for clinical AI.
FDA clearance is required for AI tools that function as software as a medical device (SaMD), meaning tools that inform or support clinical diagnosis or treatment decisions. Administrative AI applications (revenue cycle, scheduling, back-office automation) do not require FDA clearance. Tools like ChatGPT are not FDA-cleared for clinical use. Specific diagnostic AI tools for diabetic retinopathy or CT scan interpretation have clearance, but those clearances are tool-specific, not category-wide.
At minimum: accessible, consistently structured clinical data from your EHR, a HIPAA-compliant data pipeline between source systems and AI tooling, a data governance framework defining access controls and labeling standards, and documented integration with billing and scheduling systems for administrative use cases. Clinical AI applications add requirements for de-identified training data, demographic representation validation, and audit trail infrastructure for regulatory compliance.
Bias in healthcare AI is a documented patient safety issue, not a theoretical concern. AI systems trained on unrepresentative patient populations produce systematically worse outcomes for underrepresented demographic groups. Address it by requiring demographic performance breakdowns from vendors before deployment, building bias monitoring into your production model infrastructure, and prioritizing tools validated on patient populations similar to yours. Regulatory guidance now requires bias assessment in high-risk clinical AI submissions.
For administrative applications, ROI is measurable within the first quarter: coding accuracy rates, denial rates, claims processing time, scheduling no-show rates, and contact center deflection volume all have established baselines and direct revenue or cost implications. For clinical AI, the measurement horizon is longer and the metrics are different: diagnostic accuracy, time to treatment, clinical trial enrollment rates, patient outcomes. Establish baseline measurements for every application before deployment, not after.
Adoption follows trust, and trust follows transparency. Clinical staff who understand what an AI tool does, what it doesn't do, and how its outputs are validated adopt faster than those handed a new system without context. The EHR implementation experience of the 2010s left justified skepticism. Health systems that address this directly, with specific workflow integration and honest communication about model limitations, see materially better adoption outcomes.
Yes, but integration complexity varies significantly by EHR vendor and application type. Administrative AI tools (coding automation, revenue cycle, scheduling) have well-established integration patterns with major EHR platforms. Clinical AI tools require deeper integration and more rigorous validation. Plan for integration work as a first-order deployment task, not an implementation detail. Health systems that treat EHR integration as solved before it's been scoped miss their Day 30 production targets.




.avif)